Mothers
What Is Hypoxia in Babies? Causes, Types & Early Warning Signs
Apr 16 • 11 min read
Table of Content
Types of Hypoxia in Infants
What Causes Hypoxia in Babies?
Before Birth (Prenatal Causes)+
During Birth (Perinatal Causes)
After Birth (Postnatal Causes)
First
Hypoxia Symptoms in Infants: Complete Guide
1. Cyanosis (Blue or Grey Skin)
2. Respiratory Distress
3. Abnormal Heart Rate
4. Poor Muscle Tone (Hypotonia)
5. Altered Responsiveness
6. Feeding Difficulties
7. Abnormal Temperature Regulation
Effects of Hypoxia in Newborns
Mild to Moderate Hypoxia
Severe or Prolonged Hypoxia
Hypoxia vs. Anoxia: Key Differences
How
What monitoring actually does for parents and caregivers
Here is why that matters in the context of hypoxia:
What to look for in a
When to Call a Doctor Immediately
Can Hypoxia in Infants Be Prevented?
FAQs About Hypoxia in Babies
1. What is the difference between hypoxia and hypoxemia in newborns?
2. What is the first sign of hypoxia in a newborn?
3. Can a baby recover fully from hypoxia?
4. How is hypoxia in infants different from SIDS?
Key Takeaways
Hypoxia in newborns is a medical condition where the body’s tissues do not receive enough oxygen to function properly. The term comes from the Greek words hypo (under) and oxys (oxygen). In simple terms, the baby’s cells are being starved of the oxygen they need to survive and grow.
In newborns, this is particularly dangerous because their organs, especially the brain, are in a critical phase of development. Even brief periods of low oxygen can disrupt brain cell function within minutes.

Key fact: The brain consumes roughly 20% of the body’s total oxygen supply. In a newborn, whose brain is developing rapidly, hypoxia can cause irreversible damage within 4 to 6 minutes if left untreated.

Hypoxia in infants is different from anoxia, which means a complete absence of oxygen. Hypoxia refers to reduced oxygen levels, a spectrum that ranges from mild to severe.
Types of Hypoxia in Infants
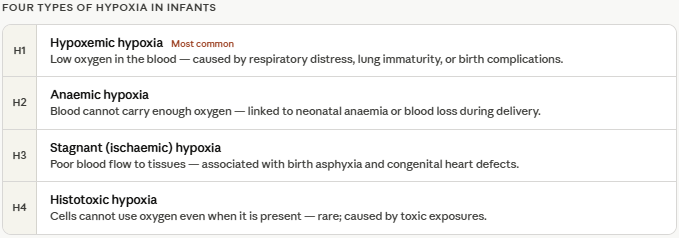
Understanding the type of hypoxia helps doctors identify the root cause and choose the right treatment. There are four main types:
Type | What Happens | Common Cause in Infants |
Hypoxemic Hypoxia | Low oxygen in the blood | Respiratory distress, lung immaturity |
Anaemic Hypoxia | Blood cannot carry enough oxygen | Neonatal anaemia, blood loss |
Stagnant (Ischaemic) Hypoxia | Poor blood flow to tissues | Birth asphyxia, heart defects |
Histotoxic Hypoxia | Cells cannot use oxygen | Rare; toxic exposures |
The most common type in newborns is hypoxemic hypoxia, often linked to underdeveloped lungs, respiratory infections, or complications during birth.
What Causes Hypoxia in Babies?
Hypoxia in newborns can develop before birth (prenatal), during labour and delivery (perinatal), or after birth (postnatal). Here is a breakdown of the most common causes:
Before Birth (Prenatal Causes)+
Placental insufficiency — when the placenta fails to deliver adequate oxygen to the foetus
Umbilical cord compression or prolapse — reduces blood and oxygen flow
Maternal anaemia or low blood pressure — limits the oxygen available for transfer to the baby
Preeclampsia or gestational hypertension — impairs placental function
Foetal growth restriction (FGR) — associated with chronic oxygen deficiency in the womb
During Birth (Perinatal Causes)
Prolonged or obstructed labour — increases the risk of oxygen deprivation
Cord entanglement (nuchal cord) — the umbilical cord wraps around the baby’s neck
Placental abruption — the placenta separates from the uterine wall prematurely
Maternal haemorrhage — reduces oxygen delivery to the baby
Neonatal birth asphyxia — a direct cause of perinatal hypoxia
After Birth (Postnatal Causes)
Respiratory distress syndrome (RDS) — especially in premature infants whose lungs are not fully mature
Meconium aspiration syndrome — when the baby inhales meconium (first stool) into the lungs
Transient tachypnoea of the newborn (TTN) — faster-than-normal breathing that reduces oxygen intake efficiency
Congenital heart defects — structural heart problems that reduce oxygen circulation
Neonatal sepsis — infections that compromise respiratory and cardiovascular function
Pneumonia — lung infection causing poor gas exchange
Apnoea of prematurity — pauses in breathing common in premature babies
First Signs of Hypoxia: What to Watch For
The first sign of hypoxia in a newborn is often a change in skin colour; specifically, a bluish or greyish tint around the lips, mouth, or fingertips. This is called cyanosis, and it occurs when deoxygenated blood circulates near the skin’s surface.
However, cyanosis may not always be immediately visible, particularly in babies with darker skin tones. In those cases, parents and caregivers should also watch for:
Rapid or laboured breathing — nostrils flaring, belly breathing, or visible effort to breathe
Grunting sounds with each breath — a sign the baby is trying to keep the airways open
Unusual limpness or low muscle tone (hypotonia) — the baby feels floppy when held
A weak, high-pitched, or absent cry — different from the baby’s normal cry
Poor feeding or sucking — the baby lacks the energy or coordination to feed properly
Pale, mottled, or ashen skin — especially on the face, hands, and feet
Early recognition matters. Research indicates that identifying and treating neonatal hypoxia within the first hour of onset significantly reduces the risk of long-term neurological complications. If you notice any of these signs, seek emergency medical care immediately.
The challenge for most parents is that these early signs can be subtle, and they don’t always appear when you’re awake and watching. A baby’s oxygen level can drop silently during sleep, during a feed, or in those long, quiet hours when you’re finally resting too. That’s why continuous monitoring of SpO2 (blood oxygen saturation) and pulse rate has become one of the most recommended for newborn care, especially in the days and weeks after coming home from the hospital.
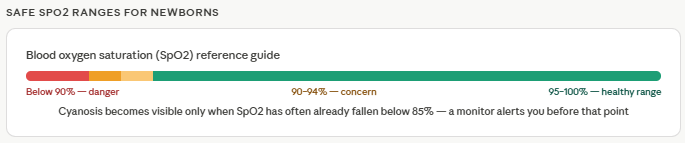
A wearable pulse oximeter designed for newborns typically worn on the foot or wrist can track SpO2 and heart rate around the clock and alert you the moment readings fall outside safe ranges. For a healthy newborn, SpO2 should consistently stay between 95–100%. A reading that dips below 90% is a signal that something needs attention, even if your baby looks calm. Having a device that catches that drop in real time rather than waiting for visible symptoms — is the difference between reacting to a crisis and preventing one.
Hypoxia Symptoms in Infants: Complete Guide
1. Cyanosis (Blue or Grey Skin)
Cyanosis is the hallmark symptom of hypoxia in infants. It appears as a blue, grey, or dusky discolouration of the skin, particularly around the mouth (perioral cyanosis), lips, and nail beds. Central cyanosis affects the lips and tongue more seriously than peripheral cyanosis (tips of fingers and toes) and requires immediate attention.
Note: Acrocyanosis (blue hands and feet only) is normal in the first 24–48 hours after birth. Central cyanosis is not.
2. Respiratory Distress
Watch for these specific breathing abnormalities:
Tachypnoea: Breathing rate above 60 breaths per minute
Nasal flaring: Nostrils widening with each breath
Grunting: A low sound made on exhalation to maintain lung pressure
Chest retractions: The skin between or below the ribs pulls inward with each breath
Apnoea: Episodes where breathing stops for more than 20 seconds
3. Abnormal Heart Rate
Both bradycardia (heart rate below 100 bpm) and tachycardia (heart rate above 160 bpm at rest) can indicate hypoxia. A healthy newborn’s resting heart rate is typically between 120–160 beats per minute.
Heart rate and oxygen saturation are closely linked — when SpO2 drops, the heart compensates by beating faster. This is why devices that monitor both parameters together give a more complete picture than relying on visual observation alone.
4. Poor Muscle Tone (Hypotonia)
A baby with hypoxia may feel unusually floppy or limp. This is known as neonatal hypotonia and is a significant red flag during newborn assessments (it directly impacts the Apgar score).
5. Altered Responsiveness
Difficulty waking the baby or keeping them alert
Reduced or absent response to light, sound, or touch
Seizure-like movements or abnormal jerking in severe cases
6. Feeding Difficulties
Hypoxic babies often cannot coordinate the suck-swallow-breathe pattern required for feeding. Poor feeding in the early days, especially combined with other symptoms, warrants a medical evaluation.
7. Abnormal Temperature Regulation
Hypoxic newborns may have difficulty maintaining body temperature, appearing cold to touch or experiencing temperature fluctuations.
Effects of Hypoxia in Newborns
The effects of hypoxia in newborns depend on the severity, duration, and timing of oxygen deprivation. Here is what can happen across the spectrum:
Mild to Moderate Hypoxia
Temporary breathing difficulties that resolve with supplemental oxygen
Short-term feeding challenges
Possible minor developmental delays, often manageable with early intervention
Severe or Prolonged Hypoxia
When oxygen deprivation is significant or goes untreated, the consequences can be serious and long-lasting:
Organ System | Potential Long-Term Effect |
Brain | Hypoxic-Ischaemic Encephalopathy (HIE), cerebral palsy, cognitive delays, epilepsy |
Heart | Persistent pulmonary hypertension, cardiac dysfunction |
Kidneys | Acute kidney injury, long-term renal impairment |
Gut | Necrotising enterocolitis (NEC) in premature infants |
Lungs | Chronic lung disease, bronchopulmonary dysplasia |
Hypoxic-Ischaemic Encephalopathy (HIE) is the most serious consequence of neonatal hypoxia. It occurs when both oxygen and blood flow to the brain are reduced. HIE affects approximately 2–3 per 1,000 live births in high-income countries, and the rate is significantly higher in low- and middle-income settings.
The good news: When hypoxia is detected early and treated with therapeutic hypothermia (cooling therapy) within 6 hours of birth, outcomes for babies with moderate HIE improve significantly.
Hypoxia vs. Anoxia: Key Differences
| Hypoxia | Anoxia |
Definition | Reduced oxygen supply to tissues | Complete absence of oxygen |
Severity | Ranges from mild to severe | Severe by definition |
Onset | Can be gradual or sudden | Usually sudden |
Common Cause in Newborns | Respiratory distress, birth complications | Total cord occlusion, cardiac arrest |
Outcome | Reversible if treated quickly | Higher risk of permanent injury |
How Continuous Oxygen Monitoring Helps Manage Hypoxia Risk
Understanding hypoxia symptoms is important. But being able to detect a drop in oxygen before symptoms become visible is what makes the real difference especially at night, during sleep, or in those early weeks at home when you’re still learning your baby’s normal patterns.
This is where continuous SpO2 monitoring becomes genuinely useful for at-risk newborns.
What monitoring actually does for parents and caregivers
A small wearable sensor placed on your baby’s foot or wrist uses pulse oximetry — the same technology used in hospitals to continuously measure two things: blood oxygen saturation (SpO2) and heart rate. The data is typically sent wirelessly to an app on your phone, giving you a real-time view of your baby’s vitals whether you’re in the same room or not.
Here is why that matters in the context of hypoxia:
It catches the drop before the symptoms show. Cyanosis (blue skin) typically becomes visible only when SpO2 has already fallen significantly — often below 85%. A monitor will alert you when levels dip below a set threshold (usually 90–94%), giving you a window to act before it becomes an emergency.
It removes the guesswork during sleep. Neonatal apnoea — pauses in breathing that can reduce oxygen levels — happens most often during sleep. Without continuous monitoring, these episodes can go unnoticed until the baby is in distress.
It supports parents of high-risk newborns. Premature babies, babies who experienced birth complications, or those with known respiratory or cardiac conditions are at elevated risk of hypoxia. For these families, continuous monitoring at home is not just reassurance — it is an active safety measure.
It helps you share accurate data with your doctor. If your baby has had an episode of low oxygen, having a recorded log of SpO2 and heart rate trends means your paediatrician can see exactly what happened and when — rather than relying on a description of symptoms you observed.
What to look for in a newborn oxygen monitor
If your doctor recommends monitoring your baby’s oxygen levels at home, or if your baby was born prematurely or had a difficult birth, here are the features that matter:
Continuous SpO2 and pulse rate tracking — not just spot checks
Adjustable alerts for low oxygen (below 90%) and abnormal heart rate
Designed for newborn skin — soft, lightweight, and non-irritating
Wireless and app-connected — so you can see readings without disturbing the baby
Movement tracking — to distinguish between true low-oxygen events and motion artefacts
Data history — so you can review trends and share reports with your healthcare provider
For hospitals: In NICU and PICU settings, continuous neonatal vital sign monitoring — including SpO2, respiratory rate, and heart rate — is standard protocol for managing hypoxia and preventing deterioration in at-risk newborns.
When to Call a Doctor Immediately
Seek emergency medical care immediately if your baby shows any of the following:
Blue or grey colour around the lips or mouth
Breathing rate consistently above 60 per minute
Grunting, chest retractions, or nasal flaring
Limp body or unresponsiveness
A seizure or shaking episode
Temperature below 36°C or above 38°C in a newborn under 3 months
Absence of breathing for more than 10 seconds
Do not wait to see if the symptom resolves on its own. Neonatal hypoxia is a time-sensitive emergency.
Can Hypoxia in Infants Be Prevented?
While not all cases of hypoxia can be prevented, several evidence-based strategies reduce risk significantly:
During Pregnancy: - Regular antenatal check-ups to monitor foetal growth and wellbeing - Continuous foetal heart rate monitoring (cardiotocography/CTG) during high-risk pregnancies - Managing maternal conditions like anaemia, hypertension, and gestational diabetes
During Labour: - Electronic foetal monitoring to detect early signs of foetal distress - Prompt management of prolonged or obstructed labour - Avoiding unnecessary cord clamping immediately after birth
After Birth: - Immediate newborn assessment using the Apgar score - Neonatal resuscitation protocols for babies born in poor condition - Continuous vital sign monitoring for premature or at-risk newborns - Pulse oximetry screening before hospital discharge - Ongoing SpO2 and heart rate monitoring at home for babies with known risk factors — using a wearable newborn pulse oximeter that tracks oxygen levels continuously and alerts caregivers to drops in real time
Want to know more about the specific signs of low oxygen in babies and how to monitor your newborn at home? Read our detailed guide: Signs of Low Oxygen in Babies: How to Spot Hypoxia Before It Becomes an Emergency
FAQs About Hypoxia in Babies
1. What is the difference between hypoxia and hypoxemia in newborns?
Hypoxemia refers specifically to low oxygen levels in the blood (measured by SpO2 or blood gas). Hypoxia is a broader term that refers to insufficient oxygen at the tissue level. Hypoxemia often leads to hypoxia, but not always immediately.
2. What is the first sign of hypoxia in a newborn?
The first visible sign of hypoxia in a newborn is often cyanosis — a bluish or greyish discolouration around the lips and mouth. In babies with darker skin, look for changes in the colour of the gums, inside of the mouth, or around the eyes. Rapid or difficult breathing often accompanies early hypoxia.
3. Can a baby recover fully from hypoxia?
Recovery depends on the severity and duration of oxygen deprivation. Mild hypoxia that is treated quickly often has no long-term effects. Severe or prolonged hypoxia, particularly if it causes HIE, can result in permanent neurological impairment. Early intervention, including therapeutic hypothermia, significantly improves outcomes.
4. How is hypoxia in infants different from SIDS?
Hypoxia is a condition with identifiable symptoms and causes. Sudden Infant Death Syndrome (SIDS) occurs suddenly and unexpectedly, without prior warning signs. However, some cases of SIDS may involve an inability to respond to low oxygen levels during sleep.
What oxygen level is dangerous for a newborn?
An SpO2 reading below 90% is considered dangerously low for a newborn. Healthy newborns should maintain SpO2 levels of 95–100% after the first 10 minutes of life. Premature infants are often maintained at 90–95% to prevent complications from excess oxygen
Key Takeaways
Hypoxia in newborns occurs when body tissues don’t receive enough oxygen and requires immediate medical attention.
The most common early signs are cyanosis (blue or grey skin around the lips), laboured breathing, and limpness.
Causes range from umbilical cord complications and placental insufficiency before birth to respiratory distress syndrome and infections after birth.
Severe hypoxia can cause Hypoxic-Ischaemic Encephalopathy (HIE), cerebral palsy, and other long-term neurological conditions.
Early detection and treatment — within the first hour — dramatically improves outcomes.
Regular antenatal monitoring and foetal heart rate assessment remain the most effective prevention tools.